Authors – Dianne Edmonds and Marietta Mehanni – ePublication of Australian Fitness Network – Resources Library.
By breaking the silence around pelvic floor issues and instructing your aqua participants in suitable exercises, you can improve knowledge about, and function in, this often neglected area, write Dianne Edmonds and Marietta Mehanni.
Many people who want to exercise without the implications of impact, joint stress, post-exercise muscle soreness and overheating issues choose to exercise in water. However, this client group is often also the one most challenged by pelvic floor issues.
It is well known that mature adults, and certainly menopausal or post-menopausal women, would also prefer to exercise in water because of issues with ‘wetting themselves’ during land-based exercise. Pregnant women and obese clients also prefer to exercise in water for the obvious reduced impact benefit, but also because the pelvic floor is more protected in water. Lower back pain is also strongly linked with pelvic floor weakness, and there is an awareness that aqua aerobics provides a safer choice of fitness program for participants wanting to protect their backs.
| MORE ‘FLOOR’ |
|---|
| For more information on implementing a program of pelvic floor-safe exercise progressions, read ‘Inspiring confidence: pelvic floor fitness for your clients’ by Troy Morgan and Carol Archer. Simply enter ‘Inspiring confidence’ into the Site Search field at the bottom of this page. |
It is clear, then, that aqua aerobics not only holds massive appeal for these population groups, but also posesses many benefits related to pelvic floor issues. This provides aqua aerobic instructors with a huge opportunity to provide much needed education, information and instruction on what the pelvic floor is, and how it can be ‘used’ during the workout.
MEET THE PELVIC FLOOR
The pelvic floor lies at the bottom of the bony ring of the pelvis, and consists of muscles, nerves, and vascular and fascial tissues that form a dynamic structure with the roles of:
- Maintaining a ‘normal level’ of resting tone and contracting to maintain bladder and bowel control (the loss of which is called incontinence)
- Relaxing to allow the passing of urine, wind and faeces
- Sexual responsiveness, and potentially playing a role in the generation of an orgasm
- tretching to allow the movement of a baby down the birth canal
- Supporting the pelvic organs, which are the bladder, uterus in women, and bowel (when the organs are not supported and drop down within or even outside of the vaginal opening in women, this is called a prolapse).
Research shows that:
- One in three women who have ever had a baby wet themselves.
- Up to 50 per cent of women trying to do pelvic floor muscle exercises from a pamphlet or brief verbal instruction get the technique wrong.
- 30 to 43 per cent of women with urge incontinence or prolapse ‘bear down’ or strain when attempting to lift the pelvic floor muscles.
- Given this fact, it is important that you don’t assume that all of your clients are doing their pelvic floor exercises correctly, even when you give them clear instructions.
- A BMI of less than 25 is desirable to reduce the risk of incontinence.
PELVIC FLOOR MUSCLES AS PART OF THE ‘CORE’
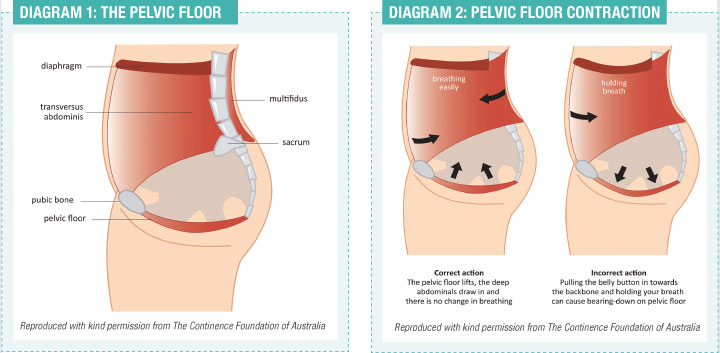
The pelvic floor muscles also form the base of the group of muscles known as the ‘deep core’. The deep core can be likened to a cylinder comprised of: transverse abdominus (front), multifidus (back), diaphragm (top) and the pelvic floor muscles (base). The function of the deep core is to stabilise and support the spine and control the pressure inside the abdomen.
If the muscles of the deep core work together well, the pelvic floor muscles lift, the abdominal and back muscles draw in to support the spine and breathing should be easy (Diagram 2: Correct action).
If an exercise is performed with poor technique, or the load is too high, the deep core may not work properly. For example, if an aqua client is using buoyancy equipment where the resistance is too strong for their level of pelvic floor muscle fitness, their pelvic floor muscles may be unable to respond correctly. If they hold their breath or draw their abdomen in without lifting the pelvic floor muscles first, this may also put extra pressure on the pelvic floor (Diagram 2: Incorrect action). Over time, repeated occurrence of this pressure during an exercise session may place strain on the pelvic organs, potentially resulting in loss of control over the bladder or bowel, or a prolapse.
TEACHING CORRECT PELVIC FLOOR TECHNIQUE
To ensure your aqua clients are correctly activating their pelvic floor muscles, they must first be exercising with the lumbar spine in a neutral position. Then, a ‘lifting up and holding’ action is required through the pelvic floor. Clients need to have continual reminders and instruction about what an accurate pelvic floor contraction is, so that they don’t hold their breath or bear down while they exercise.
In aqua classes pelvic floor muscle exercises can be included in standing, during cool down, stretching or postural awareness components.
Verbal cueing phrases that can be used in an aqua class include:
‘Focus on lifting up your pelvic floor on the inside’
‘Drawing up inside, tightening around your front and back passages’
‘Imagine you are holding onto a full bladder and wind at the same time’ (in whatever way you feel most comfortable saying this)
Another way to cue is to also suggest what not to do:
‘Breathe, don’t suck in the ribs and upper abdominal area (under the ribcage)’
‘Avoid strongly pulling your belly button towards your spine or bracing – this is too strong’
When the pelvic floor and the transversus abdominus are working well with correct ‘patterns of recruitment’ then they should work together. Descriptions to explain this to participants may include:
‘The pelvic floor and lower abdominals are wired up to work together’
‘They work best when they work together’.
Between contractions, advise participants that it is OK to feel their lower abdominals gently tighten, but that they shouldn’t feel tightening under their ribs or in their upper abdominal area.
Hold times for contractions can vary from two to three seconds up to five to 10 seconds, although long holds may mean the clients will cool down in the pool environment.
You also need to emphasise relaxation;
‘When you relax you should feel your pelvic floor muscles release completely’. If they don’t feel a relaxation, either their pelvic floor muscles have fatigued and relaxed already, or they may still be holding them tightly and therefore need to focus on relaxing between the contractions. To check if the muscles are fatiguing, clients can do a shorter contraction, e.g. two to three seconds, and if they then feel the muscles relax, they will gain the awareness of their own pelvic floor muscle hold time, and be able to work on gradually increasing that hold time.
LAND VS. WATER
The effect of buoyancy decreases the gravitational forces acting through the pelvis during aquatic exercise, and therefore decreases the pressure on the pelvic floor compared with similar exercise performed on land. In fact, buoyancy does not simply affect the force of the internal organs on the pelvic floor, it also ‘floats’ the internal organs, so even jumping and jogging exercises that would not usually be recommended for land-based workouts are appropriate in the water. This is of particular benefit for pregnant or obese participants.
FAST VS. SLOW
There are marked differences in pelvic floor response to a fast jog and a slow jog. Similar differences are also evident in other exercises, such as cross country ski, jumping jacks and kicks. When these classic aqua moves are performed with speed and, consequently, more turbulence, the pelvic floor responds by lifting and engaging with the transverse abdominus to create a stable torso. Slower rebounding actions create more force on the pelvic floor, and thus cause more pelvic floor stress.
BUOYANCY EQUIPMENT
Buoyancy equipment, such as dumbbells, noodles and kickboards, are predominantly used for buoyancy-resisted and buoyancy-supported exercises. Buoyancy-resisted exercise is when the buoyant tool is pushed down into the water or kept submerged while performing various shallow or suspended exercises. Often, participants hold their breath and thus bear down onto their pelvic floor when performing buoyancy-resisted exercises, which is problematic if pelvic floor weakness exists. This inappropriate use of the core muscles could actually contribute to pelvic floor weakness.
Correct breathing is an essential component when performing buoyancy-resisted exercises. Forced exhalation is required when the buoyant equipment is pressed downward, and inhalation when the tool is released to the surface. When the buoyant tool is submerged for a lengthy period of time to either suspend the body or to develop muscle endurance, breathing cues are extremely important. The verbal cues need to be graduated and layered slowly to ensure that participants are not overwhelmed with information.
Buoyancy-supported exercise is when the body is fully supported by the buoyant tool. This method is most often used for suspended exercises and is the recommended alternative to buoyancy-resisted suspended exercises. Buoyancy-supported exercises provide the opportunity for clients to focus on recruiting the pelvic floor and breathing correctly while performing the exercises. When using dumbbells and noodles for these exercises, the tools need to be held under the armpits, below the buttocks or between the legs, as gripping with the hands may encourage some participants to hold their breath, thus defeating the purpose of performing buoyancy-supported exercises.
SPREAD THE WORD
Because they are hidden from view, it is not easy for women to know whether their pelvic floor muscles are working correctly. Many women don’t seek help for the problems associated with a weak pelvic floor because they are embarrassed, think that it is normal, and/or don’t know that treatment is available. As an aqua fitness instructor who includes pelvic floor muscle exercises in your fitness program, you can also advise women where to seek help if they do have a problem. Free brochures are available from the Continence Foundation of Australia, and the free call number for the National Continence Helpline is 1800 33 00 66, where clients can be referred to a Continence Health Professional in their area, if necessary.
Images courtesy of the Continence Foundation of Australia pelvicfloorfirst.org.au
| REFERENCES: |
|---|
| Bump, R C; Hurt, G; Famtl, A and Wyman, J (1991). ‘Assessment of kegel pelvic floor muscle exercise performance after brief verbal instruction’. American Journal of Obstetrics and Gynaecology. 322-329.Sapsford, R R, Hodges, P W, Richardson C A, Cooper, D H, Markwell, S J and Jull, G A (2001). ‘Co-activation of the abdominal and pelvic floor muscles during voluntary exercises’. Neurourology & Urodynamics, 20, 31-42.Thompson, J.A., O’Sullivan, P.; Briffa, K.; and Neumann, P. ‘Assessment of pelvic floor movement using transabdominal and transperineal ultrasound’. International Urogynecology Journal 2005; 16: 285-292.Thompson, J.A., O’Sullivan, P.; Briffa, K.; and Neumann, P (2006). ‘Differences in muscle activation patterns during pelvic floor muscle contraction and Valsalva manouevre’. Neurourology & Urodynamics, 25, 148-155. |